 |
Case Report
Primary osteosarcoma of the breast: A case report
1 Resident, Department of Anatomopathology, Ibn Rochd University Hospital Center, Hassan II University of Casablanca, Faculty of Medicine and Pharmacy, Casablanca, Morocco
2 Professor, Department of Anatomopathology, Ibn Rochd University Hospital Center, Hassan II University of Casablanca, Faculty of Medicine and Pharmacy, Casablanca, Morocco
3 Resident, Department of Gynecology and Obstretrics, Ibn Rochd University Hospital Center, Hassan II University of Casablanca, Faculty of Medicine and Pharmacy, Casablanca, Morocco
4 Professor, Department of Gynecology and Obstretrics, Ibn Rochd University Hospital Center, Hassan II University of Casablanca, Faculty of Medicine and Pharmacy, Casablanca, Morocco
5 Professor and Chief of Anatomopathology Department, Department of Anatomopathology, Ibn Rochd University Hospital Center, Hassan II University of Casablanca, Faculty of Medicine and Pharmacy, Casablanca, Morocco
Address correspondence to:
Evrard Niyonkuru
Casablanca,
Morocco
Message to Corresponding Author
Article ID: 100011P03EN2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Niyonkuru E, Regragui M, Sami Z, Nihad DSF, Elkarroumi M, Karkouri M. Primary osteosarcoma of the breast: A case report. Edorium J Pathol 2021;7:100011P03EN2021.ABSTRACT
Introduction: Primary osteosarcoma of the breast is an extremely rare malignant tumor, and only few cases have been reported in the literature. It is a rare histological type of all breast tumors. Primary osteosarcoma of the breast is considered to be an aggressive tumor with a poor prognosis.
Case Report: We report a case of primary osteosarcoma of the breast in a 71-year-old woman. The patient presented a lump in the left breast, discovered on self-examination. Ultrasound and mammographic data revealed a large solid and cystic mass in the left breast, graded as highly suggestive of malignancy (Breast Imaging and Reporting Data System [BI-RADS] category 5). After a tru-cut biopsy showing a malignant mesenchymal tumor proliferation, the patient has undergone a mastectomy. The histological examination of the mastectomy specimen revealed the presence of sarcomatous proliferation with abundant osteoid substance and chondroid area but no epithelial component. The diagnosis of primary osteosarcoma of the breast was determined after ruling out the primary differential diagnosis, metaplastic carcinoma, by an immunohistochemical study. Immunohistochemically, tumor cells were non-reactive with anti-cytokeratin antibodies.
Conclusion: It is essential to recognize this rare and aggressive pathologic tumor variant in order to manage patients suffering from this pathology appropriately.
Keywords: Breast cancer, Histology, Mastectomy, Primary osteosarcoma
INTRODUCTION
Primary osteosarcomas of the breast are very rare, aggressive, and heterogeneous neoplasms derived from non-epithelial elements of the gland and represent less than 1% of breast cancers and less than 5% of all sarcomas [1].
Its unusual presentation in the breast can put the pathologist in the dilemma of diagnostic. We report the case of a 71-year-old woman who was diagnosed with a primary osteosarcoma in her left breast. Through this case and review of the literature, we highlight several details of this rare histological type of breast cancer.
CASE REPORT
A 71-year-old woman, with no specific history, who presented with a lump in the left breast, discovered on self-examination, progressing gradually for one year. She was in good general condition with no other associated symptoms. The clinical examination showed a 7 cm mobile rounded mass in the outer quadrant of the left breast, without skin retraction and no palpable axillary lymph nodes (Figure 1).
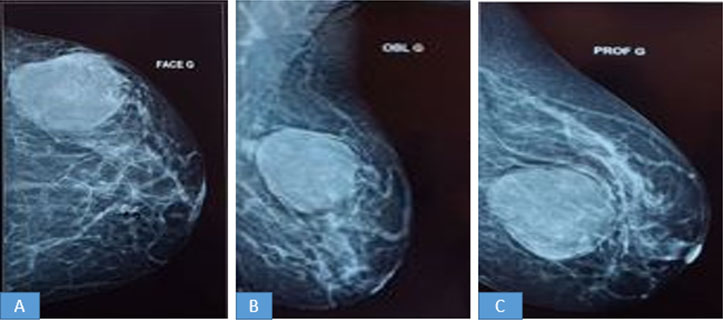
Mammography revealed a voluminous dense opacity, focally with indistinct margin, containing microcalcifications in the outer quadrants of the left breast (Figure 2).
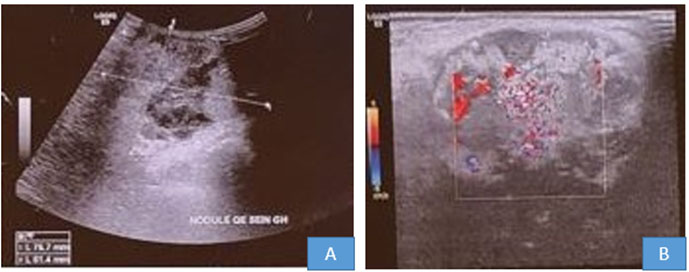
Ultrasonography (US) showed a large solid and cystic mass with indistinct margin containing microcalcifications, measuring 77 mm × 62 mm. Doppler evaluation demonstrated surrounding vascularity (Figure 3). The lesion was graded as highly suggestive of malignancy (Breast Imaging and Reporting Data System [BI-RADS] category 5).
A tru-cut biopsy was taken, which showed a malignant mesenchymal tumor proliferation, suggesting a fibro-chondro-osteosarcoma. The patient underwent a mastectomy.
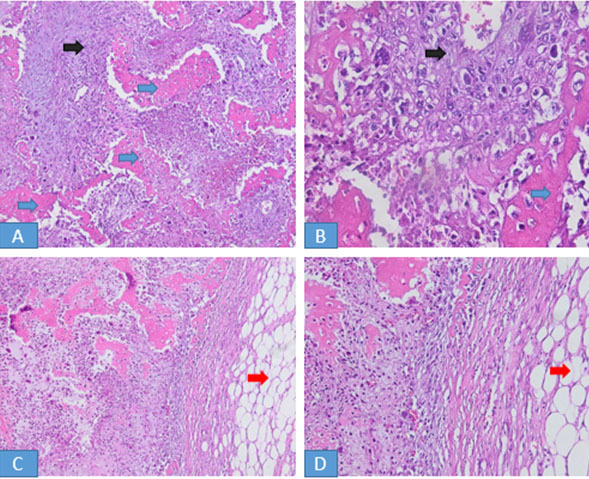
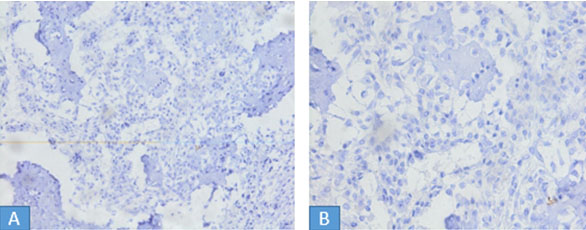
The gross examination of the specimen from the left breast revealed a white beige neoplasm, well-circumscribed, firm, measuring 14×9×5.5 cm, focally hemorrhagic and necrotic (Figure 4). The histological examination showed a malignant spindle cell tumor with abundant osteoid substance and chondroid area. There were scattered multinucleated osteoclastic tumor giant cells. The carcinomatous component was not found (Figure 5). Multiple sections were taken to detect an epithelial component, thus ruling out the possibility of a metaplastic carcinoma. The immunostaining for cytokeratine AE1–AE3 showed no epithelial component (Figure 6).


DISCUSSION
Carcinoma is the most common malignancies of the breast and sarcomas form a minority of breast neoplasms. Primary sarcomas of the breast account for <1% of all primary breast malignancies [2]. Among those, osteosarcoma is extremely rare.
Approximately, 150 cases of this pathology have been reported in the literature since 1957 [1]. The histogenesis of primary breast osteosarcoma remains unclear. Still, an evolution from totipotent mesenchymal cells of the breast stroma or a transformation from a preexisting fibroadenoma or phyllodes tumors have been suggested [1],[3].
The presentation of breast osteosarcoma usually occurs at an advanced age, in contrast with skeletal osteosarcomas where the patients are younger. The majority of the cases are in patients that are over 60 years old with a reported median age of 64.5 years [2]. Risk factors for extraskeletal osteosarcomas have not been identified to date, although some instances have been attributed to local irradiation, trauma, or the presence of a foreign body [2].
The present patient was 71 years old with no history of trauma or irradiation, no tumor in other sites. Clinically, breast osteosarcomas often present as rapidly enlarging masses. Rarely, patients report associated bloody nipple discharge or nipple retraction [4].
Mamographically, these tumors often present as well circumscribed, dense lesions within the breast parenchyma, with focal or extensive coarse calcifications [3],[5].
The border may be regular or irregular. The mammographic appearances may be deceptively benign and may imitate a benign fibroadenoma in a third of cases [2]. The most common macroscopic finding is the neoplasm well circumscribed, which joins the appearance found in the present case.
In almost every case in the literature, the diagnosis of primary osteocarcoma was established histologically [6]. Histologically, this tumor is indistinguishable from the conventional osteosarcomas of the bone or other extraskeletal ones [3]. The diagnosis criteria of primary breast osteosarcoma include the absence of a tumor bone, the presence of the osteoid substance or bony streaks and the lack of an associated epithelial tumor component [2]. The absence of the epithelial component must be confirmed by immunohistochemical study or by ultrastructural study [7]. In our patient, the diagnosis of primary osteosarcomas of the breast was established on the morphology by the absence of an epithelial component and confirmed by negative staining with cytokeratin antibody (AE1/AE3). The principal histological differential diagnosis in our case was metaplastic carcinoma [1]. However, this was excluded because of negative epithelial markers on immunohistochemical staining.
Malignant phyllodes with osteosarcomatous differentiation can be also raised as the differential diagnosis. The treatment is surgical by a complete removal of the tumor with negative margins or a mastectomy. An axillary lymph node dissection is essentially not indicated because an axillary node involvement is exceptional [8].
In the present case, axillary lymph node dissection was not performed.
The role of adjuvant therapy is unclear because of limited data and his efficacy has not been well established [9].
Primary osteosarcomas of the breast have a poor prognosis with a high possibility of recurrence and metastasis, especially by hematogenous route instead of lymphatic spread. The most common distant site for metastasis are the lungs [2]. Silver et al. in their study of 50 patients with primary breast osteosarcoma reported a 5-year survival of 38%, with 28% of patients developing local recurrence and 41% with distant metastases [2].
CONCLUSION
It is essential to be aware of this unusual pathologic tumor variant and to differentiate it from metaplastic carcinoma. An early diagnosis, confirmed by an immunohistochemical study and a rapid treatment mainly surgical, is necessary to improve the prognosis, which remains very poor despite everything.
REFERENCES
1.
Khan S, Griffiths EA, Shah N, Ravi S. Primary osteogenic sarcoma of the breast: A case report. Cases J 2008;1(1):148. [CrossRef]
[Pubmed]

2.
Silver SA, Tavassoli FA. Primary osteogenic sarcoma of the breast: A clinicopathologic analysis of 50 cases. Am J Surg Pathol 1998;22(8):925–33.
[Pubmed]
3.
Bahrami A, Resetkova E, Ro JY, Ibañez JD, Ayala AG. Primary osteosarcoma of the breast. Report of 2 cases. Arch Pathol Lab Med 2007;131(5):792–5. [CrossRef]
[Pubmed]
4.
Thomas KA, Roy N, Troxell M, Oh KY. Osteosarcoma of the breast. Breast J 2014;20(2):204–6. [CrossRef]
[Pubmed]
5.
Ribeiro-Silva A, Zambelli Ramalho LN, Zucoloto S. Phyllodes tumour with osteosarcomatous differentiation: A comparative immunohistochemical study between epithelial and mesenchymal cells. Tumori 2006;92(4):340–6.
[Pubmed]
6.
Oluwasola AO, Adebamowo CA, Ezeome ER, Oduntan O, Akang EE. Osteogenic sarcoma in the breast—Case report of a diagnostic dilemma. Afr J Med Med Sci 2001;30(1–2):129–31.
[Pubmed]
7.
Going JJ, Lumsden AB, Anderson TJ. A classical osteogenic sarcoma of the breast: Histology, immunohistochemistry and ultrastructure. Histopathology 1986;10(6):631–41. [CrossRef]
[Pubmed]
8.
Ciatto S, Bonardi R, Cataliotti L, Cardona G. Sarcomas of the breast: A multicenter series of 70 cases. Neoplasma 1992;39(6):375–9.
[Pubmed]
9.
Momoi H, Wada Y, Sarumaru S, et al. Primary osteosarcoma of the breast. Breast Cancer 2004;11(4):396–400. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Evrard Niyonkuru - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Meriem Regragui - Conception of the work, Design of the work, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Zineb Sami - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Da Silva Fidélia Nihad - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mohamed Elkarroumi - Conception of the work, Design of the work, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mehdi Karkouri - Conception of the work, Design of the work, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Evrard Niyonkuru et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.

